Jerold S Bell DVM, Dept. of Clinical Sciences, Tufts Cummings School of Veterinary Medicine, N. Grafton, MA USA jerold.bell@tufts.edu
(Lecture presented at the World Small Animal Veterinary Association 2021 Virtual World Congress 13 Nov. 2021)
This WSAVA Lecture is also available as a PDF. WSAVA21 Degenerative Myelopathy.pdf
Table of Contents
DEGENERATIVE MYELOPATHY-DIAGNOSIS AND INHERITANCE
Degenerative myelopathy (DM) is a specific, infrequently encountered, fatal inherited disorder of slowly progressive spinal cord degeneration in dogs. It affects both sexes equally. Dogs present five years of age or older; with an average of nine years. Dogs from smaller-statured breeds tend to have a later onset. Progression to euthanasia or death usually occurs over six months to one year, however affected dogs supported with a wheel-cart and excellent supportive care can sometimes be maintained longer. It presents most commonly in German Shepherd Dogs and Boxers. It is sporadically seen in Pembroke Welsh Corgis, Cardigan Welsh Corgis, Bernese Mountain Dogs, Rhodesian Ridgebacks, Borzoi and Chesapeake Bay Retrievers. It is rarely diagnosed in other breeds or mixed-breed dogs. Diagnosis can only be confirmed on post-mortem histopathological examination of the spinal cord. The biggest issue with DM is misdiagnosing it in a dog affected with another treatable or non-fatal disease.
CLINICAL SIGNS
Based on Dr. Joan Coates’ findings at the University of Missouri in the USA there are 4 stages of degenerative myelopathy:
Stage 1: Asymmetric, general proprioceptive ataxia and spastic paresis in the pelvic limbs. Intact spinal reflexes.
Stage 2: Non-ambulatory paraparesis, paraplegia. Reduced to absent pelvic limb spinal reflexes. Pelvic limb muscle atrophy ± urinary/fecal incontinence.
Stage 3: Flaccid paraplegia, thoracic limb paresis. Absent spinal reflexes. Severe pelvic limb muscle atrophy. Urinary/fecal incontinence.
Stage 4: Flaccid tetraplegia. Severe generalized muscle atrophy. Dysphagia, dystonia, respiratory difficulty.
Clinically we usually only see Stage 1 DM; an upper motor neuron (UMN) disease relating to the T3-L3 spinal cord. In dogs that can be maintained in Stage 2 with hind limb paralysis (in a wheel cart or recumbency) the disease can progress to LMN signs. However this is extremely rare to encounter in practice as most clients opt for euthanasia when they become nonambulatory.
Stage 1 clinical signs of DM are insidious, and owners may not seek veterinary attention for some time – thinking they are age-related or due to arthritis. A significant signalment with DM is there is no pain or hyperesthesia. DM first presents with pelvic limb ataxia and paresis. With progression, knuckling of the hind paws, dragging of the toes (with associated wearing of the nails), dysmetria, crouching in the hind limbs and crossing of the hind limbs can occur. Swaying of the hind end and falling if forced to turn quickly can occur with gaiting. The clinical signs affect both hind limbs, although there can be asymmetry in their severity. Urinary and fecal incontinence do not occur in Stage 1, although dogs with progressive disease can lose their housetraining if they cannot get outside or position themselves for elimination. They can develop a UMN bladder. Hind limb muscle atrophy in Stage 1 is from disuse and not neurogenic. In Stage 2 and later stages, the signs can progress to the forelimbs, and in the end-stages can cause flaccid tetraparesis and affect the muscles of respiration and elimination.
In Stage 1 DM there is deficient hind limb proprioceptive placing and hopping, and deficient extensor thrust. Pain and withdrawal responses are normal. Crossed extensor reflexes may be present. Patella reflexes are usually normal to exaggerated. Occasionally there can be a diminished patella reflex, but this would relate to involvement of the dorsal roots of the femoral nerve (afferent), and not lower motor neuron (LMN) involvement. Panniculus response remains intact. Anal and tail tone remain normal.
DIFFERENTIAL DIAGNOSIS
There are many causes for hind end weakness in dogs. Most of the differentials to DM occur at much higher frequency and importantly many are treatable or non-fatal diseases. Differentials include; significant hip dysplasia, type II intervertebral disc disease, discospondylitis, myelitis, spinal neoplasia (intra or extra medullary), cauda equina syndrome, fibrocartilaginous embolic myelopathy (FCEM), spinal arachnoid diverticula, and other rare or sporadically occurring myelopathies. Other diseases that may initially affect the pelvic limbs include caudal cervical spondylomyelopathy, and generalized neuromuscular, infectious, toxic, metabolic, ischemic and inflammatory diseases.
Dural ossification and spondylosis can be a common finding in older dogs and should not be labeled as the cause for neurologic signs without further workup. As an important non-painful differential, FCEM is peracute, non-progressive and can affect anal and tail function. Myelography or MRI rules out compressive spinal cord disease. CSF analysis in DM is usually normal. Electrophysiologic testing is normal – signifying normal motor reflex pathways. MRI may rarely show spinal cord changes but is more useful to rule out other disease. Caution must be advised in over interpreting diagnostic findings as many of the differentials can be comorbidities with DM.
A clinical diagnosis of degenerative myelopathy is only offered based on; ruling out other causes of non-painful spinal cord disease, observing the expected progression of clinical neurological deterioration, disease in a recognized susceptible breed, and a homozygous sod1 genetic test result. If a genetic test for the sod1 variant is not homozygous “at risk” this rules out DM as a differential. However, a homozygous “at risk” result is NOT diagnostic and should NOT be used to confirm a diagnosis of DM.
Histopathological findings show degeneration of the myelinated axons in all funiculi, but especially in the dorsolateral funiculi in the T3-L3 segments. Pathognomonic to DM are cytoplasmic aggregates of sod1 in neurons identified through immunohistochemical staining with anti-sod1 antibodies.
The high rate of sod1 DM genetic testing has put the term degenerative myelopathy into common conversation. This has caused great confusion in differentiating other diseases, as well as damage to breed gene pools from inappropriate selection against the sod1 variant. There are many disorders affecting the spinal cord that can be classified as degenerative (progressive) myelopathies (spinal cord diseases). To avoid confusion, the term degenerative myelopathy should be used exclusively for (sod1) DM as first described by Averill in German Shepherd Dogs in 1973.
TREATMENT
DM is a fatal disease. Medical therapy does not relieve the clinical symptoms. As arthritis is often a comorbidity, a trial of NSAIDs should be offered to patients with presumptive DM. Steroids do not affect progression of DM and usually cause issues with polydipsia and polyuria. Physical therapy and exercise to maintain muscle tone and to slow atrophy are important supportive measures. Response to supplements and alternative therapies are anecdotal and lack controlled studies.
GENOMICS
The mode of inheritance of DM has always been considered to be complex – involving more than one gene pair. In 2009, Drs. Gary Johnson & Joan Coates (UMo) discovered a sod1 liability gene that must be present for clinical disease to occur. Almost all histopathologically confirmed cases of DM are homozygous for the sod1 variant. In only the Bernese Mountain Dog, there is a low-frequency second variant in the sod1 gene and if a BMD is being tested it should be for both variants.
Exacerbating the issue with sod1 variant testing is that it is the most frequent mutation found in genetic testing of all dogs; at a frequency of 7.77% in mixed-breed dogs and 5.41% in purebred dogs (identified in over 120 breeds). This indicates that the sod1 variant is an ancestrally ancient mutation that originated and was disseminated from a dog that existed long before the separation of breeds. The frequency of the sod1 variant is over 20-90% in more than 30 breeds, although no dogs in most of these breeds have ever been confirmed with DM.
Canine DM is an animal model for human amyotrophic lateral sclerosis (ALS; Lou Gehrig’s disease). In ALS over 25 identified genetic mutations cause disease liability; including many mutations in the sod1 gene. Over ninety percent of all cases of ALS are sporadic with no identified genetic mutation – indicating personal mutations causing the disease. The difference between sod1 homozygous “at risk” dogs that do not develop clinical disease, and dogs with clinical DM may be due to additional unidentified genetic mutations. Infrequent clinical diagnoses of DM in other breeds should be considered sporadic due to personal mutations, and not breed-related disease.
Drs. Coates and Johnson’s research in Pembroke Welsh Corgis identified a mutation in the SP110 gene that is present in 40% of DM confirmed dogs, but only in 4% of unaffected dogs, and causes an earlier age of onset. This variant has not been found in other breeds, nor has a commercial test been developed. Other research into the genetic cause of clinical DM in the German Shepherd Dog is being studied at the University of Uppsala in Sweden.
Drs. Coates and Johnson find that the sod1 variant has age related penetrance and hypothesize that most dogs do not live long enough to develop clinical signs. Their research has identified histopathologically affected dogs from 34 breeds and mixed-breed dogs. However, in the vast majority of these often-populous breeds there are only one or a handful of cases. They have also identified a low number of sod1 variant heterozygous (carrier) dogs with pathologically confirmed DM. In man, sod1 DM is a dominantly inherited disease.
While data show that an increasing number of sod1 homozygous dogs develop clinical DM as they age, the evidence is not there that DM is a monogenic disease only involving the sod1 gene. Based on testing frequencies in mixed breed and purebred dogs that live well into their teens, veterinarians should be diagnosing hundreds of thousands of DM affected dogs every year, as opposed to the infrequent diagnoses that are observed. The vast majority of dogs with hind end weakness or spinal cord signs have diagnostic “mimics” to clinical sod1 DM. There is a difference between diagnoses confirmed by specialists researching the disease versus cases seen in routine clinical practice. Realistically in practice, all clinically diagnosed affected dogs will be in the expected breeds (primarily GSD and Boxers) and will test homozygous for the sod1 variant. Otherwise, other diagnoses must be pursued.
CORRELATING sod1 TESTING WITH CLINICAL DISEASE
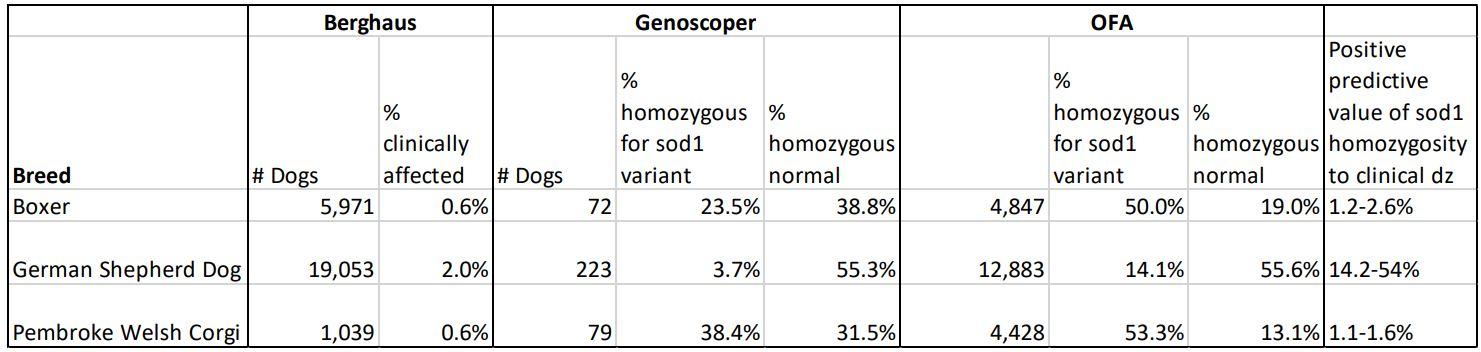
It is difficult to determine the penetrance of homozygous sod1 testing to dogs clinically affected with DM. Clinical DM has only been pathologically confirmed in 34 of over 120 breeds identified with the sod1 variant. The only published study of clinically diagnosed DM was by Dr. Roy Berghaus at UC-Davis, of diagnoses at US veterinary teaching hospitals between 1990- 1999. Two sources of worldwide testing frequencies for the sod1 variant are published data by Mars/Genoscoper and data on the OFA website. The following table summarizes the compiled data.

It is obvious that even in breeds with pathological confirmation of clinical disease; the variant frequency is exponentially higher than the frequency of clinically affected dogs, and the homozygous state has low penetrance and is poorly predictive of clinical disease.
GENETIC COUNSELING
Degenerative myelopathy is not a treatable disease, and no intervention will alter its fatal outcome. The high gene frequency of the sod1 variant across breeds and the infrequent clinical presentation of DM in any breed causes much confusion in genetic counseling. With public acceptance of direct-to-consumer multiplex panel genetic testing for dogs, all panel tests include sod1 variant test results regardless of their relevance to individual breeds and dogs. In all breeds (and mixed-breed dogs) a DM “at risk” result places a significant and unnecessary emotional burden on owners who believe that their family member will develop DM and die from the disease – which is highly unlikely to occur. A decision to euthanize a dog due to a DM “at risk” test result when differentials include common treatable diseases such as disc disease and musculoskeletal disease are unacceptable and borders on malpractice.
The greatest issue with the misuse of sod1 genetic test results (both in breeds with and without confirmation of affected DM dogs) is where breeders are devastating their gene pool diversity by selecting against the sod1 variant. In many breeds, heterozygous carriers and homozygous “at risk” dogs represent the majority of the breed. The only situation where sod1 test results should be considered in making treatment and breeding decisions is when there are close relatives confirmed with clinical DM (and therefore a high probability of carrying other unidentified but necessary mutations for clinical disease).
While the sod1 variant is the most frequent DNA variant identified in dogs, clinical degenerative myelopathy needs to be put back in the RARE and INFREQUENTLY DIAGNOSED category where it belongs.
SELECTED REFERENCES
Averill DR Jr. Degenerative myelopathy in the aging German Shepherd dog: clinical and pathologic findings. J Am Vet Med Assoc. 1973 Jun 15;162(12):1045-51. https://pubmed.ncbi.nlm.nih.gov/4196853/
Awano T, Johnson GS, Wade CM, et. al. Genome-wide association analysis reveals a SOD1 mutation in canine degenerative myelopathy that resembles amyotrophic lateral sclerosis. Proc Natl Acad Sci U S A. 2009 Feb 24;106(8):2794-9. https://doi.org/10.1073/pnas.0812297106
Brown RH, Al-Chalabi A. Amyotrophic Lateral Sclerosis. N Engl J Med. 2017 Jul 13;377(2):162-172. https://doi.org/10.1056/nejmra1603471
Coates JR, March PA, Oglesbee M, et. al. Clinical characterization of a familial degenerative myelopathy in Pembroke Welsh Corgi dogs. J Vet Intern Med. Nov-Dec 2007;21(6):1323-31. https://doi.org/10.1892/07-059.1
Coates, J.R., Wininger, F.A. Canine degenerative myelopathy. Vet. Clin. North Am. Small Anim. Pract. 2010, 40, 929–950. https://doi.org/10.1016/j.cvsm.2010.05.001
Donner J, Anderson H, Davison S, et. al. Frequency and distribution of 152 genetic disease variants in over 100,000 mixed breed and purebred dogs. PLoS Genet 2018, Apr 30;14(4):e1007361. https://doi.org/10.1371/journal.pgen.1007361
OFA - The Canine Health Information Center. Breed Statistics: Degenerative Myelopathy. https://www.ofa.org/diseases/breed-statistics?disease=DM. Last accessed 13 Nov. 2021.
Zeng R, Coates JR, Johnson GC, et. al. Breed distribution of SOD1 alleles previously associated with canine degenerative myelopathy. J Vet Intern Med. Mar-Apr 2014;28(2):515-21. https://doi.org/10.1111/jvim.12317
(Revised Nov. 2021)
Also see DogWellnet Blogs:
Correcting the confusion around degenerative myelopathy - Dr. Brenda Bonnett
Infographic - Quick Facts on Degenerative Myelopathy and Genetic Testing
HGTD this week - BRR Updates on sod-1-Testing for Degenerative myelopathy-DM
 Donate
Donate

Recommended Comments
There are no comments to display.
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.
Note: Your post will require moderator approval before it will be visible.